Peritoneal dialysis is usually self administered. In both hemodialysis and peritoneal dialysis, the blood is cleansed. However, in peritoneal dialysis the process takes place within the patients own body, in the peritoneal or abdominal cavity, rather than outside the body in a machine. The peritoneum is a thin membrane which covers the intestines and other contents of the abdominal cavity. During dialysis, the dialysate is introduced into the abdominal cavity, allowed to stay in for some time, and then drained out. The peritoneum basically functions the same as the semipermeable membrane used in the artificial kidney machine. Since it contains a whole network of tiny blood vessels called capillaries, the peritoneum is constantly able to provide a new supply of blood to be filtered. As blood flows through the peritoneum, waste products are filtered (through diffusion) and excess fluids are removed (through osmosis). The wastes flow into the dialysate which remains or dwells within the abdominal cavity for a variable period of time. At the end of this period the dialysate is drained from the abdomen and fresh dialysate is introduced.
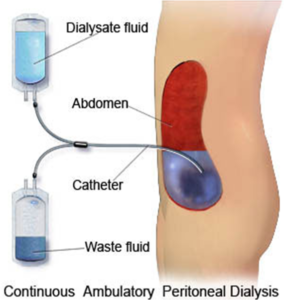

Figure: CAPD access site
Access for peritoneal dialysis:
Access for peritoneal dialysis is gained via a flexible hollow tube, called a catheter, which is surgically implanted through the wall of the abdomen into the abdominal cavity. This catheter is usually permanent, but may be replaced as needed. A potential problem with peritoneal dialysis is peritonitis, an infection of the lining membrane of the peritoneal cavity. The exchanges of dialysis fluid must be performed using sterile technique in order to prevent this type of infection.
Depending on the way peritoneal dialysis is performed it is described in two different ways:
- Continuous Ambulatory Peritoneal Dialysis (CAPD)
- Continuous Cycling Peritoneal Dialysis (CCPD)
Continuous Ambulatory Peritoneal Dialysis
Continuous Ambulatory Peritoneal Dialysis (CAPD) is self administered and machine free. CAPD exchanges are performed in a clean, private location where the patient is comfortable. The process of exchanging the dialysis fluid is repeated every 4 to 6 hours during the day, with each exchange taking approximately 30 minutes (10 minutes to introduce and 20 minutes to drain the dialysate). Each day, the final dialysis is performed right before the patient goes to bed at night. Since the patient is continually dialyzing, there are usually fewer dietary restrictions. CAPD provides mobility for the patient, and thus an improved quality of life. It also provides flexibility of timing so that the patient can be restored to near normal life.On an average three bags are used per day.
The details of an exchange are as follows:
Fluid that has been dwelling in the peritoneal cavity needs to be removed so fresh fluid may be infused and the blood cleansing process can continue. The catheter is attached to a Y SET. This Y set has a drain bag on one end and a fresh bag of dialysate on the other. For outflow, the empty bag is placed on the floor and the used fluid is allowed to drain into it by gravity. When the bag is full, the line is opened, clamped and the inflow line is opened. For inflow, the two litre bag of dialysate is raised above the patients shoulder and the fresh, warm dialysate is infused by gravity. When that bag is empty, the inflow line is closed and the Y set and bags are removed and discarded. The patient then resumes normal activity until it is time for another exchange.
Continuous Cycling Peritoneal Dialysis
Continuous Cycling Peritoneal Dialysis (CCPD) is very similar to CAPD, however, in this case, the exchanges are performed at night while the patient sleeps. To facilitate this process the patient is hooked up to an automatic cycling machine. This machine makes several evenly spaced exchanges during the night and a final one just before the patient gets up in the morning. During the day either one exchange or no exchanges are made. An advantage of CCPD is that the likelihood of infection caused by improper handling of the dialysis equipment is reduced. With only one hook-up per day rather than four or five there is less chance that the patient will introduce some bacteria into the peritoneal cavity; thus the likelihood of peritonitis is reduced. On the other hand, it is necessary for the patient to be attached to a machine during the night hours while the CAPD patient remains totally machine free.